Biosignals Repository
Please cite the corresponding papers if you use any dataset from this repository
HAND GESTURE RECOGNITION WITH ACOUSTIC MYOGRAPHY AND WAVELET SCATTERING TRANSFORM
Acoustic Myography Data, 8 Channels, 14 Classes
Data Source: A. H. Al-Timemy, Y. Serrestou, R. N. Khushaba, S. Yacoub and K. Raoof, "Hand Gesture Recognition With Acoustic Myography and Wavelet Scattering Transform," in IEEE Access, vol. 10, pp. 107526-107535, 2022, doi: 10.1109/ACCESS.2022.3212146.
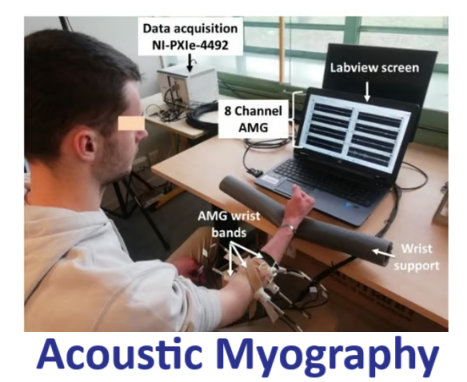
Eight high sensitivity array microphones (MPA416, BSWA technology, China) were utilised to acquire the AMG signals with a frequency range of 20Hz-20KHz, open-circuit sensitivity (50 mV/Pa)(±2dB) and inherent noise of 29dBA.The MPA416 microphones were calibrated by the manufacturer to ensure accuracy of the measurements. The MPA416 built-in Integrated Electronics Piezo-Electric (IEPE) preamplifier helps to amplify the AMG signals, to ensure a a good signal-to-noise ratio (SNR), since the amplitude of AMG signal is very low. To further ensure a low noise during AMG acquisition, the MPA416 has a low noise floor of 29 dBA. National Instruments (NI), 24-Bit PXI module for acoustic and vibration measurements (NI PXIe-4492), mounted on an NI PXIe-1073 chasse was used to perform data acquisition of 8 channels AMG at a sampling rate of 1024 Hz. A LabVIEW Virtual Instrument (VI) was developed to view the AMG signals in real-time and to save them for next parts of analysis.The subjects were asked to produce transient, moderate force contractions, that lasted 2-4 seconds. We collected AMG signals for 14 movement classes including: Pronation, Supination, Wrist Flexion, Wrist Extension, Radial Deviation, Ulnar Deviation, Hand close, Hand open, Hook grip, Fine pinch, Tripod grip, Index finger flexion, Thumb finger flexion, and No movement (Rest).
7 EMG CHANNELS, 5 LIMB POSITIONS (P1 TO P5), 8 MOVEMENT CLASSES AT EACH POSITION

TOWARDS LIMB POSITION INVARIANT MYOELECTRIC PATTERN RECOGNITION USING TIME-DEPENDENT SPECTRAL FEATURES
Data Source: R. N. Khushaba, Maen Takruri, Jaime Valls Miro, and Sarath Kodagoda, "Towards limb position invariant myoelectric pattern recognition using time-dependent spectral features", Neural Networks, vol. 55, pp. 42-58, 2014.
Variation in the limb position associated with normal use results in different EMG patterns for the same movements when carried out at different limb positions. This in turn can dramatically affect the classification accuracy of the EMG which in turns would highly affect the patients' acceptance of such myoelectrically driven prostheses. Eleven subjects, nine males and two females, aged between 20 and 37 years were recruited to perform eight classes of motion. All participants provided informed consent prior to participating in the study as was approved by the university research ethics committee. Despite the fact that the recruited subjects were all normally limbed and had no neurological or muscular disorders, one can easily notice that the same approach can be applied for transradial amputees. The main argument we are proposing here is an EMG based control scheme that is not only intended for amputees and prosthetics use but can also be applied on various EMG based control applications (including Microsoft’s muscle–computer interfaces for gaming).
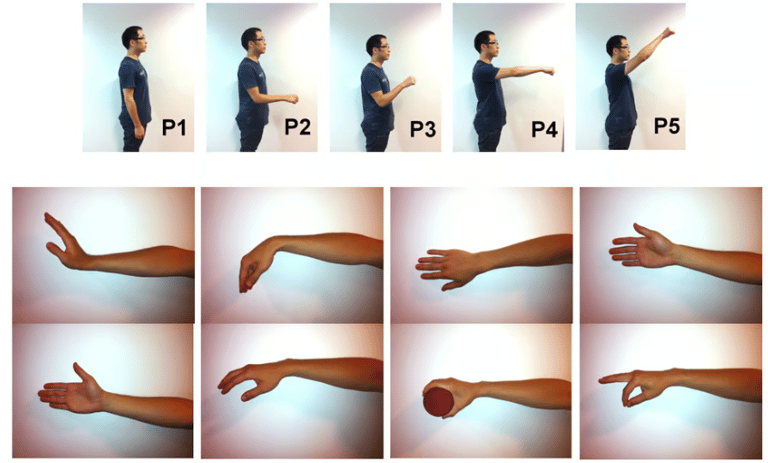
However, for transradial amputees, the muscles in the residual forearm physiologically used for flexing/extending the hand fingers and wrist are the most appropriate targets for multifingered prostheses control. Thus, the datasets were recorded using seven EMG channels (Delsys DE 2.x series EMG sensors) mounted across the circumference of the forearm and processed by the Bagnoli desktop EMG system from Delsys Inc. This in turn justifies the clinical relevance of the proposed scheme as it also applies on transradial amputees. The first EMG sensor was placed on the Palmaris Longus muscle on the right hand of each participant while the rest of the sensors were placed in a way that guarantees an equal spacing between the adjacent sensors. A 2-slot adhesive skin interface was applied on each of the sensors to firmly attach them to the skin. A conductive adhesive reference electrode, dermatrode reference electrode, was placed on the shoulder of each subject during the experiments. The collected EMG signals were amplified using a Delsys Bagnoli-8 amplifier to a total gain of 1000. A 12-bit analog-to-digital converter (National Instruments, BNC-2090) was used to sample the signal at 4000 Hz; the signal data were then acquired using Matlab software from Mathworks.1 The EMG signals were then band pass filtered between 20 and 450 Hz with a notch filter implemented to remove the 50 Hz line interference.Five different limb positions were considered in this research as shown below. The selected limb positions were chosen to cover most of the positions at which a subject may implement his/her daily activities, including situations where the test subject’s arm was hanging straight down the side (as shown in position P1), also when the arm reached forward straight (as shown in position P4), and when the arm was at an angle of 45°(as shown in position P5). There were also two possible situations between P1 and P4 (as shown in positions P2 and P3). A set of eight hand motions was performed by each subject at each of these limb positions, including: wrist flexion (1), wrist extension (2), pronation (3), supination (4), power grip (5), pinch grip (6), open hand (7), and rest (8) all shown above.
Electromyogram (EMG) Data, 8 Channels, 6 Movements Classes AND 3 Force Levels, 9 Transradial Amputees


IMPROVING THE PERFORMANCE AGAINST FORCE VARIATION OF EMG CONTROLLED MULTIFUNCTIONAL UPPER-LIMB PROSTHESES FOR TRANSRADIAL AMPUTEES
Data Source: A. H. Al-Timemy, R. N. Khushaba, G. Bugmann and J. Escudero, "Improving the Performance Against Force Variation of EMG Controlled Multifunctional Upper-Limb Prostheses for Transradial Amputees," in IEEE Transactions on Neural Systems and Rehabilitation Engineering, vol. 24, no. 6, pp. 650-661, June 2016, doi: 10.1109/TNSRE.2015.2445634.
Six movements including different grip and finger movements were investigated in the paper. These movements were discussed with some of the amputees, and they thought that they may be important to them. The gestures are: 1) Thumb flexion; 2) Index flexion; 3) Fine pinch; 4) Tripod grip; 5) Hook grip (hook or snap); 6) Spherical grip (power).To examine the effect of force variation on the performance of EMG-based PR systems, the following experimental protocol was used. After electrodes placement, each amputee was asked to examine the EMG signals on the screen in real-time and familiarize themselves with the changes in force of contraction for different movement. The objective was for them to see how the amplitude changed according to the force. They were given a couple of minutes to explore this.It is very challenging for the amputee to produce a different force level of contraction for a given movement because of the loss of visual and proprioceptive feedback from the hand after the amputation. The aim was to record lower and higher levels of force than the moderate level of force that the prosthesis usually works with. This intended to simulate the daily life scenario when the force of contraction may vary with everyday use.The amputees used their intact-hand to help them to imagine the needed movement with the required force. In addition, they used Visual Feedback (VF) from the Labview screen to see the EMG channels.
This was useful for them to produce the needed force. It is worth mentioning that TR7 had diabetes mellitus, which caused the limb to be amputated. In addition, the participant was visually impaired with little vision capability, and he did not use glasses during the experiment. Instead, he used the intact-limb to help him to imagine the needed movement.For each of the six grip patterns, the amputees produced three force levels: low, medium and high. For each force level, five to eight trials were recorded for each amputee where each trial is a holding phase lasting 8-12 seconds. Thus, the total number of trials performed by each amputee was equal to the number of movements× number of force levels ×number of trials for each movement.The following protocol was used for the recording of 3 forces levels:Low Force: To record the EMG with different forces, each amputee was asked to produce the constant non-fatiguing contraction with “low level of force”, which is lower than the usual moderate level and hold it for 8-12 seconds. It is worth noting that the amputees found the visual feedback very helpful in producing a low level of contraction. Moderate Force: In this step of the protocol, the amputees were asked to produce a moderate force level slightly higher than low level produced in the previous step, with constant non-fatiguing contraction and hold the position for a period of 8-12 seconds for each movement.High Force: A higher than moderate force level was produced by the amputees with the help of visual feedback and the intact-hand. They were instructed to produce high force level at a comfortable level to them, and to hold the contraction for 8-12 seconds. The Maximum Voluntary Contraction (MVC) was avoided since it might have caused fatigue due to the non-use of the muscle for long time. Preliminary investigation with some amputees to produce MVC for a given movement on the same day of the experiment caused some pain and fatigue. For this reason, MVC was not included in the recording protocol.
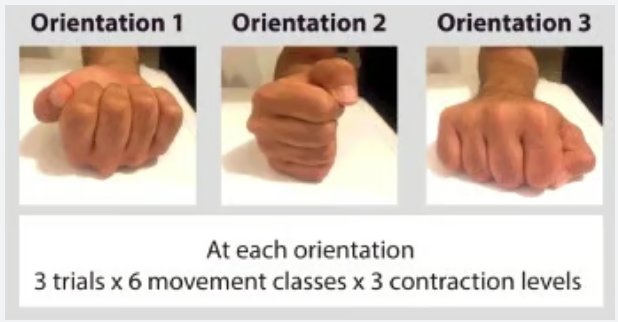
6 EMG CHANNELS, 1 ACCELEROMETER, 6 MOVEMENT CLASSES, 3 ORIENTATIONS, 3 FORCE LEVELS
IMPROVING THE PERFORMANCE AGAINST FORCE VARIATION OF EMG CONTROLLED MULTIFUNCTIONAL UPPER-LIMB PROSTHESES FOR TRANSRADIAL AMPUTEES
Data Source: R. N. Khushaba, A. Al-Timemy, S. Kodagoda, and K. Nazarpour, "Combined Influence of Forearm Orientation and Muscular Contraction on EMG Pattern Recognition", Expert Systems with Applications, vol 61, pp.154-161, 2016, open access, DOI: http://dx.doi.org/10.1016/j.eswa.2016.05.031.
Data from six EMG electrodes were recorded with a Bagnoli desktop EMG system (Delsys Inc., USA), with a gain of 1,000. Electrodes were equally spaced across the circumference of the forearm for the intact-limbed. A 2-slot adhesive skin interface was applied on each of the sensors to firmly attach them to the skin. A conductive adhesive reference electrode (dermatrode reference electrode) was placed near the subjects' wrists. An additional 3-D accelerometer (MPU-6050 from InvenSense) was attached to the participants' wrists to record wrist acceleration. A 12-bit analog-to-digital converter (National Instruments, BNC-2090) was used to sample the signal at 4,000 Hz. The accelerometer data were re-sampled to match the sampling rate of the EMG signals, with an original sampling rate of 26.6 plus-minus 0.3Hz.
Electromyogram (EMG) Data, 8 Channels, 14 Classes
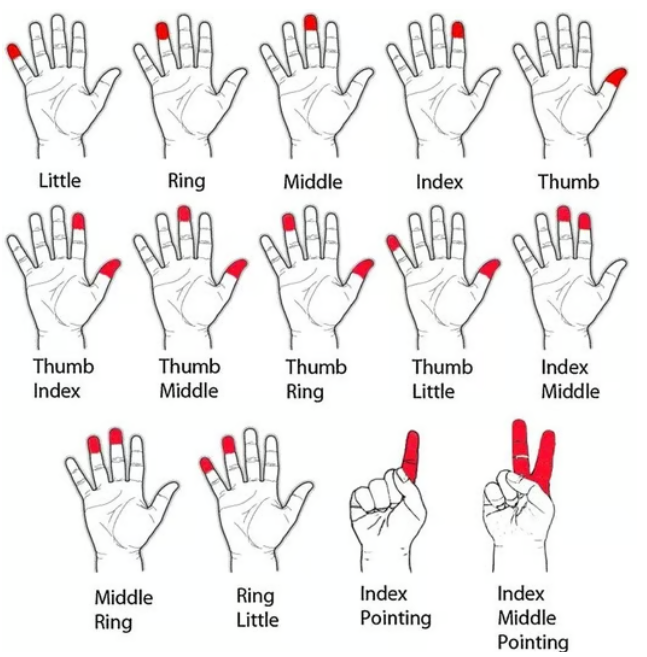
IDENTIFYING INDIVIDUAL AND COMBINED FINGERS PRESSURE ON A STEERING WHEEL
Data Source: R. N. Khushaba, S. Kodagoda, D. Liu, and G. Dissanayake, "Muscle Computer Interfaces for Driver Distraction Reduction", Computer Methods and Programs in Biomedicine, Volume 110, Issue 2 , Pages 137-149, 2013.
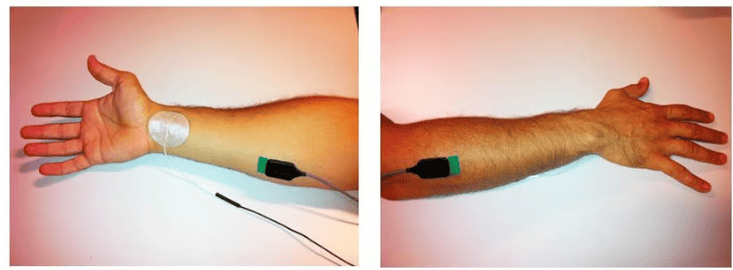
The Bagnoli desktop EMG system from Delsys Inc. was utilized to collect the EMG data during all experiments. The EMG datasets were recorded using Delsys EMG electrodes (DE 2.x series EMG sensors). The muscle-groups considered in this study were mainly the extensor and flexor muscles, as these are the muscles of interest for determining grasp and fingers movement. The extensor muscles, located on the posterior side of the forearm, extend the fingers outward as the grasp and/or finger movement initially takes a place while flexor muscles are responsible for the flexion of the finger joints. The specific extensor muscles targeted were all of the Extensor Carpi Ulnaris, Extensor Digitorum, Extensor Carpi Radialis, and Extensor Digiti Mini. On the other hand, the specific flexor muscles targeted in this paper included all of the Flexor Carpi Ulnaris, Palmaris Longus, and Flexor Carpi Radialis. Due to the layout of the different muscle in the human forearm, extra EMG electrodes were utilized to cover the circumference of the forearm to acquire, to some extent, the activity of the underlying muscles feedings the thumb and other fingers including: Flexor Pollicis longus, Extensor Pollicis Longus, and Extensor Pollicis brevis.
In total, eight EMG electrodes were mounted across the circumference of the human forearm as shown in Fig.1 (refer to paper). A 2-slot adhesive skin interface was applied on each of the sensors to firmly stick them to the skin. A conductive adhesive reference electrode, dermatrode reference electrode, was placed on the wrist of each of the subjects during the experiments. The collected EMG signals were amplified using a Delsys Bagnoli-8 amplifier to a total gain of 1000. A 12-bit analog-to-digital converter (National Instruments, BNC-2090 data acquisition board NIDAQ) was used to sample the signal at 4000 Hz; the signal data were then acquired using Matlab footnote{www.mathworks.com}. The EMG signals were then bandpass filtered between 20-450 Hz with a notch filter implemented to remove the 50 Hz line interference.
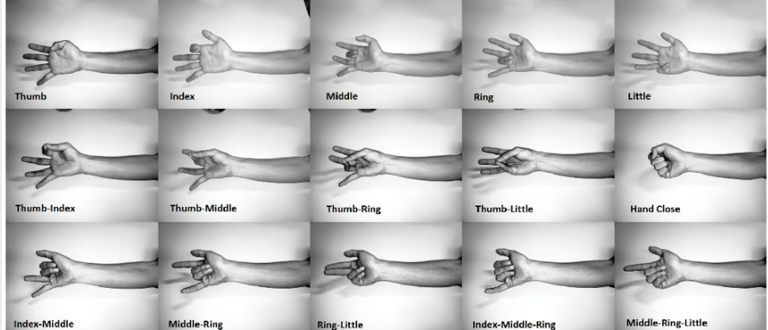
In the data collection stage, a set of eight participants (one female), aged between 20-35 years, were recruited for this experiment in which each of them had to carry out twelve classes of fingers pressures, and two fingers pointing classes, i.e., a total of 14 classes were implemented by each of the participants. All of the recruited participants were normally limbed with no neurological or muscular disorders. All participants provided informed consent prior to participating in the study. participants were seated on an armchair, facing a personal computer with a steering wheel attached on the desk as shown in Fig.2 (refer to paper). During the data collection period, both hands remained on the steering wheel in an attempt to simulate a real-world driving scenario during which the participants only had to apply some pressure on individual or combined fingers rather than performing actual gestures, except for two finger pointing classes that were performed while hands remained on the wheel. The purpose of the experiment was to show the true benefit of the muscle computer interfaces that did not require the drivers to remove their hands off the wheel, and thus providing minimally distracted driving environment. These classes included applying pressure on Thumb, Index, Middle, Ring, Little, Thumb-Index, Thumb-Middle, Thumb-Ring, Thumb-Little, Index-Middle, Middle-Ring, Ring-Little, Index Pointing, and Index-Middle Pointing as shown in Fig.ref{Hands}. Each of the aforementioned classes of fingers pressures can then be mapped to a certain function in the car, for example pressure on thumb can be used to turn on the radio or CD player, pressure on index finger can control the air conditioner, and so on. When collecting data, the participants were asked to perform each of the aforementioned fourteen movements, and hold them for a period of 5 seconds in each trial. Six trials, or repetitions, of each movement were collected. Four trials from each movement data were allocated for training and the remaining 2 trials were allocated for testing.
Electromyogram (EMG) Data, 2 Channels, 10 Classes
Data Source: R. N. Khushaba, M. Takruri, S. Kodagoda, and G. Dissanayake, "Toward Improved Control of Prosthetic Fingers Using Surface Electromyogram (EMG) Signals", Expert Systems with Applications, vol 39, no. 12, pp. 10731–10738, 2012.
Eight subjects, six males and two females, aged between 20 and 35 years were recruited to perform the required finger movements. The subjects were all normally limbed with no neurological or muscular disorders. All participants provided informed consent prior to participating in the study. Subjects were seated on an armchair, with their arm supported and fixed at one position to avoid the effect of different limb positions on the generated EMG signals (Scheme, Founger, Stavdahl, Chan, & Englehart, 2010). The EMG data was collected using two EMG channels (Delsys DE 2.x series EMG sensors) and processed by the Bagnoli Desktop EMG Systems from Delsys Inc. A 2-slot adhesive skin interface was applied on each of the sensors to firmly stick the sensors to the skin.
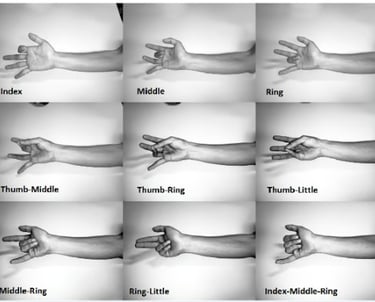
A conductive adhesive reference electrode (Dermatrode Reference Electrode) was utilized on the wrist of each subject. The positions of these electrodes are shown in Fig. 2. The EMG signals collected from the electrodes were amplified using a Delsys Bagnoli-8 amplifier to a total gain of 1000. A 12-bit analog-to-digital converter (National Instruments, BNC-2090) was used to sample the signal at 4000 Hz; the signal data were then acquired using Delsys EMGWorks Acquisition software. The EMG signals were then bandpass filtered between 20 and 450 Hz with a notch filter implemented to remove the 50 Hz line interference. Ten classes of individual and combined fingers movements were implemented including the flexion of each of the individual fingers, i.e., Thumb (T), Index (I), Middle (M), Ring (R), Little (L), and the pinching of combined Thumb–Index (T–I), Thumb–Middle (T–M), Thumb–Ring (T–R), Thumb–Little (T–L), and finally the hand close (HC) as shown in the figures within the dataset (paper also included for details).
Note: S3 and S7 were excluded from the published version, so to compare simply ignore S3 and S7.
INDIVIDUAL AND COMBINED FINGERS MOVEMENTS
Electromyogram (EMG) Data, 8 Channels, 15 Classes